
Everything OT Professionals
Need to Create Change
Earn occupational therapy CEUs, get the latest OT research, and more. Perfect for OTs, OTAs, and students from around the globe.
Or try 2 free OT CEU courses
Already a member?
Sign in here
Our AOTA-approved courses meet the requirements for NBCOT PDUs and online CEUs in all 50 states.

OT Continuing Education Courses
⭐️ New evidence taught by leading OT professionals ⭐️
Watch or listen. Then, log in to take a quiz and earn your certificate. Easy-peasy.






PEDIATRICS / ADULT REHAB / OUTPATIENT / SCHOOL-BASED / SNF / ACUTE CARE / MENTAL HEALTH / EARLY INTERVENTION / HOME HEALTH / ETHICS
Our 78 online CEU courses are presented as 1-hour episodes of the OT Potential Podcast. The first 10 minutes are spent breaking down new evidence and the remaining time is dedicated to discussing practice implications.
Meet your OT continuing education requirements for $99
📺 Get audio and video recordings for each course
✅ AOTA-approved, meets NBCOT PDU requirements,
reports to CE Broker
🎉 Meet your continued professional development (CPD) needs
📃 Download a certificate when you pass a short quiz
(15,854 certificates awarded!)
⭐️⭐️⭐️⭐️⭐️ 4.8 (2,440+ Course Reviews)
All-in-one Occupational Therapy Toolset
For OTs who truly want to transform the way they practice, staying up to date on the latest research is just the first step. That’s why we’ve built an entire suite of tools to support every facet of OT care.
Why OT Potential?
We’re not just another CEU platform.
We’re an OT-led community of occupational therapy professionals
united by our passion for using the latest OT research
to co-create the best care for our clients.
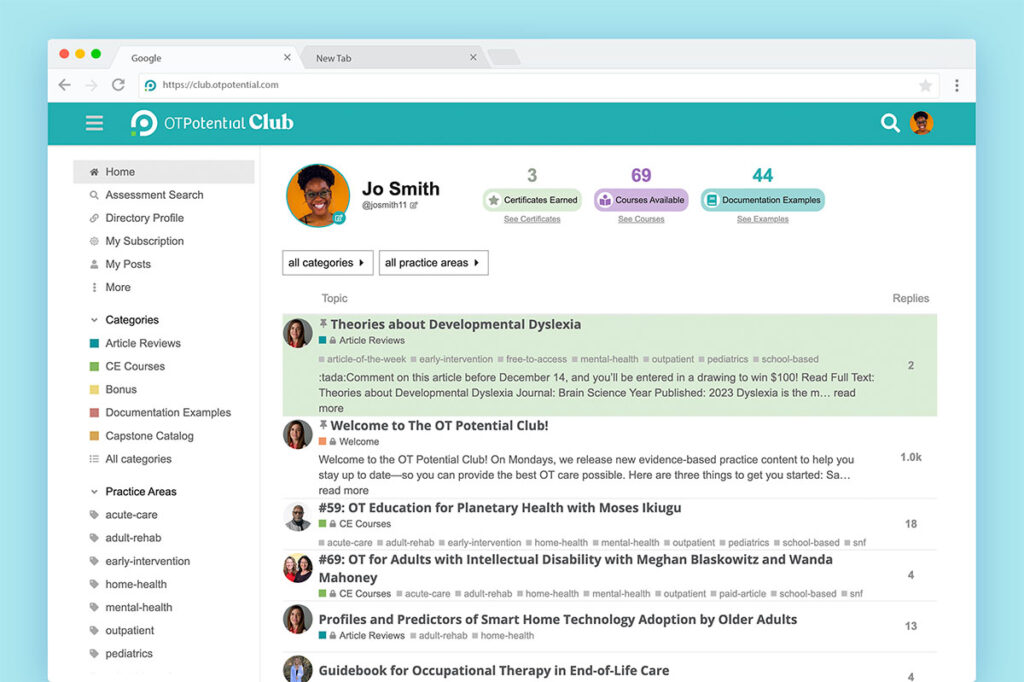
Join OT professionals from 44 countries in the
OT Potential Club
Loved by thousands of OT professionals around the world

Perpetua O.
Pediatric Private Practice Owner

Devon C.
Outpatient Adult Rehab

Laura F.
Nature-based Therapist, PhD Student

Sanchala S.
Adult Neuro, NICU, OT Educator

Jess T.
OTA, Skilled Nursing Facility

Matt B.
OT Student
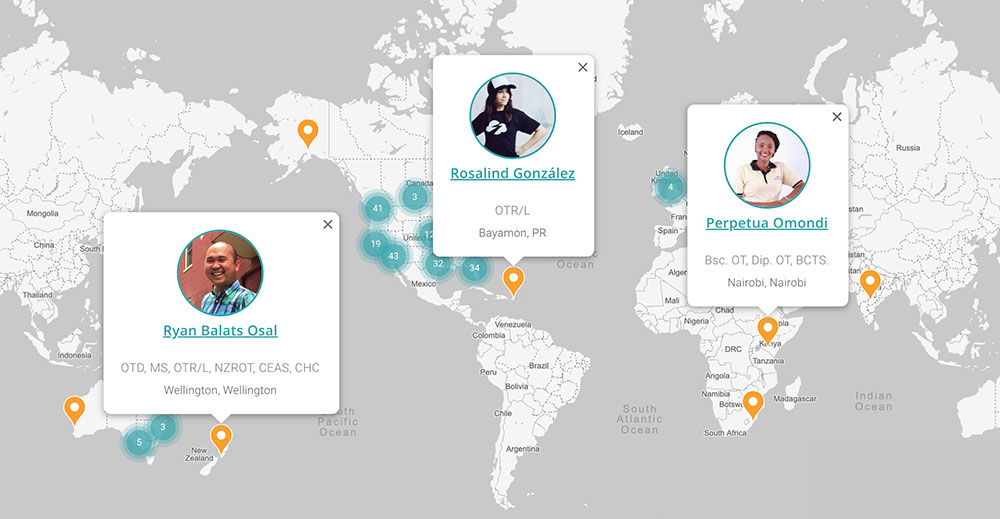
Help us put OT on the map!
Want to increase the visibility of our amazing profession online? Interested in connecting with other OTs in your location or niche? Take 5 minutes to add your profile to our searchable, public-facing OT Directory—and join our growing worldwide network of evidence-focused OTs!
Where OT students & professionals
learn new evidence together.
The research we review in OT Potential is new to ALL of us. So from the beginning, the Club has naturally been a place for students and professionals to learn alongside one another. Now, we are honored to partner with leading OT education groups to further strengthen that connection. Learn more about our school and association plans.


We make it fun and easy for OTs to connect and grow.
💜 Score a sweet member sticker just for joining the Club!
💜 Participate in research discussions (and get entered into $100 drawings for weighing in!).
💜 Get a weekly email round-up of new content and ready-to-use resources.
💜 Interact with podcast guests and fellow OTP members across the globe!

Frequently Asked Questions
Does this meet my OT CEU/PDU/CPD requirements?
All OT Potential courses are designed to meet the requirements for “online” and “independent/self-study” courses. We are AOTA-approved, and our courses also meet the requirements for NBCOT PDUs. For more details, read our blog post: Can I Earn OT CEUS from a Podcast?
To verify the CEU requirements for your specific state (within the US), check out our blog post: OT Continuing Education Explained.
Where can I listen to (or watch) the courses?
We designed our courses to live on the platforms you already use. All courses are available on Spotify, Apple, and everywhere you listen to podcasts. Courses released after June 2023 also appear on YouTube.
After watching or listening, log into the OT Potential Club to take your test, earn your certificate, and access supplemental tools and resources.
What’s included in each course?
Each 1-hour course includes:
- A written review of the research
- A podcast episode
- A YouTube video of the episode (for courses released after June 2023)
- Supplemental materials
- A quiz to earn a certificate
Many courses also feature specific assessment tools, which are added to our growing assessment search. Any accompanying documentation examples supplied by course experts are also added to our member resource library.
Which OT practice areas do you cover?
We center each course on highly-cited new research. The research often has implications spanning multiple practice areas.
To help you find the courses most relevant to you, we’ve tagged them based on applicable practice area(s): Pediatrics, Adult Rehab, Outpatient, School-based, SNF, Acute Care, Mental Health, Early Intervention, Home Health, and Ethics.
What are your accessibility features?
Courses released in June 2023 or later feature all of the accessibility features offered by YouTube, including closed captions and a live transcript. We can also generate full PDF transcripts for any of our podcast episodes by request. Simply contact us to get a copy.
When does new content come out?
In week 1 of our 2-week cycle, you’ll receive an easy-to-read journal article review based on important OT-related research. The following week, we'll release a new podcast-based course diving into that research.
How do I cancel?
Cancel your membership renewal anytime from your account settings. When you cancel, you’ll still be able to use your plan until the end of your subscription period.
If you have more questions, contact us. We’re happy to help!
Do you offer discounts?
Through February 1, 2024, you can earn a lifetime membership to OT Potential when 5 of your friends join the OT Potential Club via your unique referral link. (This discount option is being phased out in favor of discounts offered through our growing association affiliate program.)
If you have a membership to one of our partnered associations, log into your member portal to get your discount—and your association will get a cut of the sale to continue their critical advocacy work! Partnered associations include:
What if I am not 100% satisfied or renew my membership by mistake?
No problem at all! If you renew by mistake, just email us at hello@otpotential.com, and we’ll give you a full refund. If you are not 100% satisfied—and you have not completed any CEU quizzes or earned any CEU certificates—then you are also eligible for a full refund.
Get started. Pick the plan for you, and let’s create evidence-based change.
Try the Club2 OT CEU Courses and more | OT DirectoryGet Found Online | OTP Club LiteNo CEU Certificates | OT Potential Club+ CEU Certificates |
|---|---|---|---|
Free | 19 | 39 | 99 |
| Try Now Get free limited access to the OT Potenial Club for 5 days. | Join Today Essential online listing to connect with clients and OT professionals. | Join Today Perfect for students or professionals who don’t need CEU certificates. | Join Today Ideal for OTs & OTAs to earn AOTA-approved CEUs and stay up-to-date on new research. |
| Compare plans | |||
and more for free. Try now